




AA2day.org

Nerve blocks may be helpful in children undergoing VP shunt revision
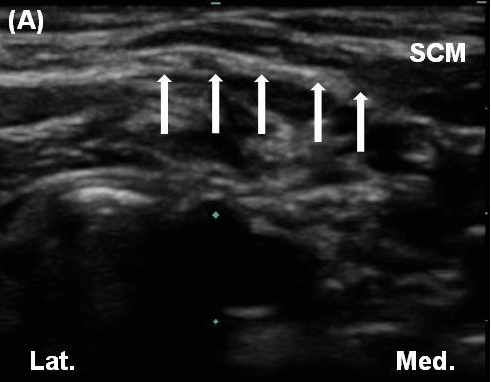
Ultrasound guidance facilitates nerve blocks that can be used for VP shunt revision. (A) Superficial cervical plexus at level of cricoid cartilage, deep to the lateral border of the sternocleidomastoid muscle. SCM – sternocleidomastoid muscle; arrows show deep border of the fascia where superficial cervical plexus is located below the lateral border of the sternocleidomastoid muscle. (Image source: A&A Case Reports)
There are many challenges for children requiring surgery, but to the extent possible pain should not be among them. In the current edition of A&A Case Reports, Drs. Michael R. King and T. Anthony Anderson, Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, Massachusetts, describe regional anesthesia in two children undergoing ventriculo-peritoneal (VP) shunt revisions. Their findings are presented in the article “Ultrasound-Guided Peripheral Nerve Blocks for Ventricular Shunt Revision in Children.â€
The first patient was a 13-year-old male who had quite a bit of pain after previous shunt revisions. For the current procedure, the occipital and cervical plexus blocks were performed after anesthesia induction. A TAP block was performed just before anesthesia emergence. For the right occipital nerve block, 5 ml 0.5% ropivacaine was deposited around the occipital nerve using ultrasound guidance; for the superficial cervical plexus block, 10 ml 0.5% ropivacaine was deposited superficially along the posterior border of the right sternocleidomastoid muscle; and for TAP block, 10 ml 0.2% ropivacaine was injected between the internal oblique and transversus abdominis using ultrasound guidance. After this procedure, postoperative pain was minimal for 16 hours, though the patient had some anxiety due to numbness over the right occiput. The mother was very satisfied with pain control for her son. The following week, the patient underwent another shunt revision where regional anesthesia was not used. Unfortunately, the patient experienced significant pain following surgery.
The second patient was a 2-year-old male and the story was similar. The patient had quite a bit of pain after previous shunt revisions. For this patient, however, a VPL rather than a VP shunt was to be placed due to abdominal infection. The authors deposited 2 ml 0.2% ropivacaine plus 3 micrograms clonidine around the right occipital nerve, 4 ml 0.2% ropivacaine plus 3 micrograms clonidine superficially along the posterior border of the right sternocleidomastoid muscle, and 2 ml 0.2% ropivacaine along the inferior portion of ribs 2 and 3 each along with 3 micrograms of clonidine. No morphine was given during the procedure. The mother reported that her child had excellent pain control for 12 hours.
Dr. Edward R. Mariano, Stanford University School of Medicine; VA Palo Alto Health Care System, Palo Alto, California, writes in the accompanying editorial titled “Peripheral Nerve Blocks in Pediatric Anesthesiology are Still Uncommon,†“I applaud the authors for their use of peripheral regional anesthesia techniques in their multimodal perioperative analgesic regimen in children and hope that more anesthesiologists caring for children will consider adopting this targeted pain management approach in the future…These benefits should not be restricted to select patients who happen to be assigned a particular anesthesiologist or have surgery on a particular day of the week or are scheduled for a particular time of the day. If providing regional analgesia is the right thing to do, it is right for all patients all the time.â€

 Visit Podcast Website
Visit Podcast Website RSS Podcast Feed
RSS Podcast Feed Subscribe
Subscribe
 Add to MyCast
Add to MyCast
{kind=link}