




Cardionerds: A Cardiology Podcast

359. Case Report: Fee-Fi-Fo-Fum: An Unusual Case of Rapidly Progressive Heart Failure – Georgetown University
CardioNerds join Dr. Ethan Fraser and Dr. Austin Culver from the MedStar Georgetown University Hospital internal medicine and cardiology programs in our nation’s capital. They discuss the following case involving an unusual case of rapidly progressive heart failure. Episode audio was edited by CardioNerds Academy Intern and student Dr. Pacey Wetstein. Expert commentary was provided by advanced heart failure cardiologist Dr. Richa Gupta.
A 55-year-old male comes to the clinic (and eventually into the hospital) for what appears to be a straightforward decompensation of his underlying cardiac disease. However, things aren’t as simple as they might appear. In this episode, we will discuss the outpatient workup for non-ischemic cardiomyopathy and discuss the clinical indicators that we as clinicians should be aware of in these sick patients. Furthermore, we will discuss the differential for NICM, the management of patients with this rare disease, and how this disease can mimic other cardiomyopathies.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.

CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
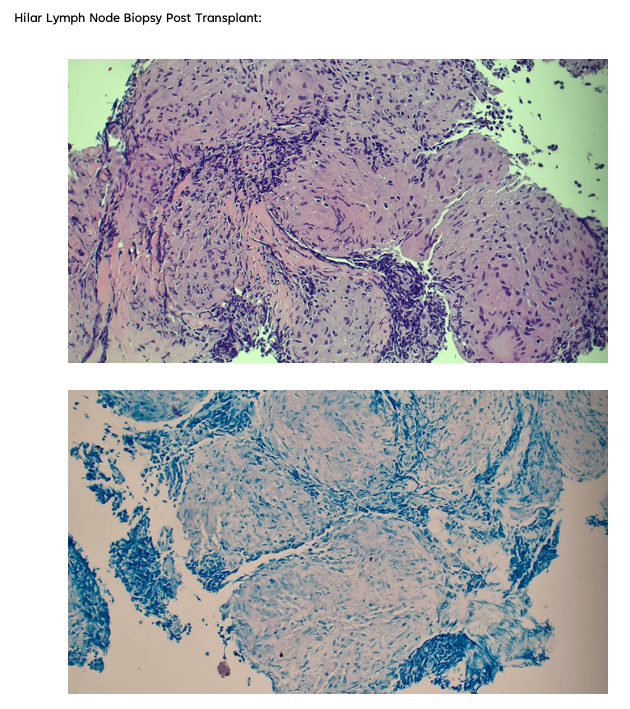
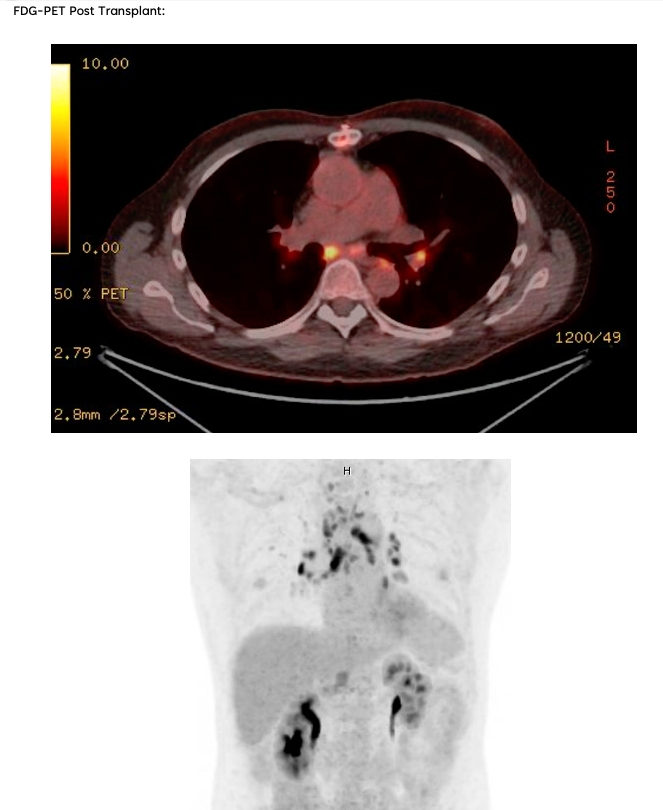
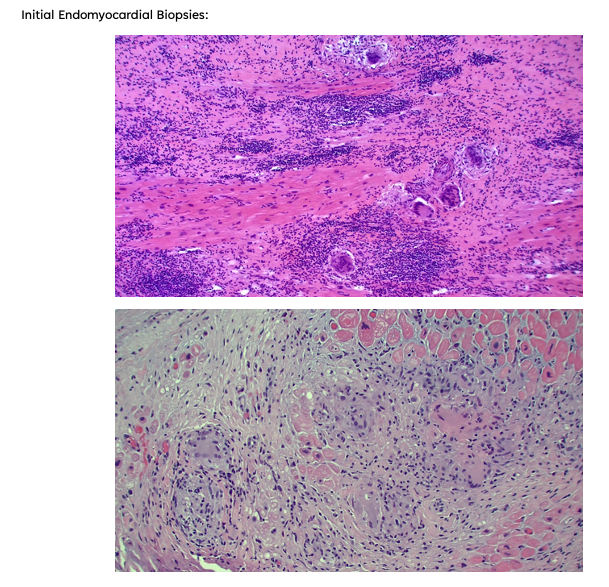
Case Media – Rapidly Progressive Heart Failure
Pearls – Rapidly Progressive Heart Failure
- The non-ischemic cardiomyopathy workup should incorporate targeted multimodal imaging, thorough history taking, broad laboratory testing, genetic testing if suspicion exists for a hereditary cause, and a deep understanding of which populations are at higher risk for certain disease states.
- Key Point: Always challenge and question the etiology of an unknown cardiomyopathy – do not assume an etiology based on history/patient story alone.
- Key Point: Always challenge and question the etiology of an unknown cardiomyopathy – do not assume an etiology based on history/patient story alone.
- Unexplained conduction disease in either a young or middle-aged individual in the setting of a known cardiomyopathy should raise suspicion for an infiltrative cardiomyopathy and set off a referral to an advanced heart failure program.
- Key Point: Consider early/more aggressive imaging for these patients and early electrophysiology referral for primary/secondary prevention.
- Key Point: Consider early/more aggressive imaging for these patients and early electrophysiology referral for primary/secondary prevention.
- Giant Cell Myocarditis is a rapidly progressive cardiomyopathy characterized by high mortality (70% in the first year), conduction disease, and classically presents in young/middle-aged men.
- Key Point: If you have a younger male with rapidly progressive cardiomyopathy (anywhere as quickly as 1-2 months, weeks in some cases) and conduction disease, consider early endomyocardial biopsy, even before other advanced imaging modalities.
- Key Point: If you have a younger male with rapidly progressive cardiomyopathy (anywhere as quickly as 1-2 months, weeks in some cases) and conduction disease, consider early endomyocardial biopsy, even before other advanced imaging modalities.
- The Diagnosis of Giant Cell Myocarditis is time-sensitive – early identification and treatment are essential to survival.
- Key Point: The median timeframe from the time the disease is diagnosed to the time of death is approximately 6 months. 90% of patients are either deceased by the end of 1 year or have received a heart transplant.
- Key Point: The median timeframe from the time the disease is diagnosed to the time of death is approximately 6 months. 90% of patients are either deceased by the end of 1 year or have received a heart transplant.
- The treatment of Giant Cell Myocarditis is still governed largely by expert opinion, but the key components include high-dose steroids and cyclosporine, largely as a bridge to transplantation or advanced heart failure therapies.
- Key Point: Multi-disciplinary care is essential in delivering excellent care in the diagnostic/pre-transplant period, including involvement by cardiology, cardiac surgery, radiology, critical care, allergy/immunology, case management, advanced heart failure, and shock teams if necessary.
- Key Point: Multi-disciplinary care is essential in delivering excellent care in the diagnostic/pre-transplant period, including involvement by cardiology, cardiac surgery, radiology, critical care, allergy/immunology, case management, advanced heart failure, and shock teams if necessary.
- There remains significant clinical overlap between Giant Cell Myocarditis and sarcoidosis, making managing equivocal cases challenging.
- Key Point: Consider early FDG-PET imaging in equivocal cases, as management during the pre-transplant period and evaluation of transplant candidacy can vary drastically between the two.
- Key Point: Consider early FDG-PET imaging in equivocal cases, as management during the pre-transplant period and evaluation of transplant candidacy can vary drastically between the two.
Show Notes – Rapidly Progressive Heart Failure
1. What is Giant Cell Myocarditis?
Giant cell myocarditis is a rare and rapidly progressive cause of heart failure due to T-cell lymphocyte mediated myocardial inflammation. The pathogenesis of GCM is incompletely understood – histologically, there is infiltration of the myocardium by T-lymphocytes and macrophages, and there is typically evidence of upregulation of IL-17 and TNF-a. Classically, the disease state is associated with electrical (e.g., ventricular tachycardia, high-grade AV block) and hemodynamic instability – all of which typically progresses rapidly over a period of weeks to months. This male-predominant disease tends to occur in young and middle-aged patients – with a mean age between 42 and 60 based on several registries. While a rare disease, a high index of suspicion is necessary when patients present with rapidly progressive or fulminant heart failure, as a missed diagnosis of giant cell myocarditis is invariably fatal. Early and rapid identification of this uniquely high-risk group of heart failure patients and prompt initiation of therapy targeted towards the underlying autoimmune process, as well as management at a center with advanced heart failure and cardiovascular ICU support, is necessary.
2. How is Giant Cell Myocarditis Diagnosed?
Establishing a diagnosis requires an endomyocardial biopsy (EMB), although EMB has imperfect sensitivity for GCM. Cardiac biomarkers and imaging serve an adjunct role in diagnosis; TTE findings can be variable, with either normal or dilated LV cavity size and increased wall thickness, which may be related to acute edema and inflammation. Worse LVEF on presentation has been shown to correlate with shorter transplant-free survival time. Troponin levels may be elevated, but case series have shown a lack of correlation between prognosis and troponin elevation in GCM, and importantly, in some cases, troponin values have been negative in patients later found to have GCM by biopsy. Advanced imaging is not always practical as these patients are often hemodynamically unstable, but CMR can demonstrate findings typical of myocarditis (i.e. the 2018 Lake Louise criteria).
3. What is the treatment for Giant Cell Myocarditis, and what are the future steps for disease management?
Cyclosporine-based combination immunosuppressive therapy, in addition to standard heart failure guideline-directed medical and procedural therapy and management of arrhythmias, can improve outcomes in these patients. Typical regimens include cyclosporine, high-dose steroids as the mainstay, and azathioprine or alemtuzumab (an anti-CD52 monoclonal antibody) as adjunctive agents. Patients are often co-managed by advanced heart failure, cardiac intensivists, and rheumatology. As the disease progresses, patients often develop sustained or symptomatic ventricular tachycardia, conduction abnormalities refractory HF with a dilated LV phenotype and many require mechanical circulatory support and/or cardiac transplantation.
GCM can remit and relapse, sometimes many years after initial diagnosis; an advanced heart failure team should follow these patients and should continue some immunosuppression (usually a calcineurin inhibitor) for at least 2 years. Overall, our understanding of the mechanism and management of GCM continues to evolve; high-grade evidence such as randomized controlled trials are extremely difficult to perform due to the rarity and high acuity of these presentations, therefore enrolling these patients in shared multicenter registries where able is essential to shrinking our knowledge gaps of this rare disease state.
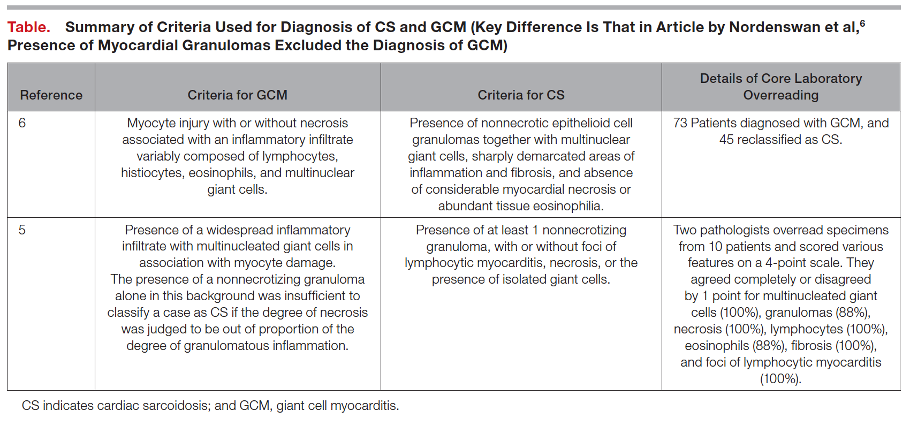
4. What else should one consider in presumed cases of Giant Cell Myocarditis?
There exists a significant clinical overlap between Giant Cell Myocarditis and Cardiac Sarcoidosis, so much so that some argue the two diseases exist on opposite ends of one disease spectrum. Both notably present with significant arrhythmia burden and advanced heart failure symptoms, although they are both treated quite differently and present with different time courses (mean time to onset of symptoms 0.3 months for GCM, 7 months for CS). Furthermore, data from Nordenswan et al. from Finland reveals that the diagnosis of GCM on histology was recategorized to CS in 62% of their studies reviewed upon secondary pathology review. To this end, it is important that clinicians consider further advanced imaging modalities (i.e., FDG-PET) in equivocal cases and consider expert pathology evaluation of endomyocardial biopsy samples as proper escalation of care and rapid identification can prevent significant treatment delays.
References – Rapidly Progressive Heart Failure
- Amancherla, Kaushik, Juan Qin, Yu Wang, Margaret L. Axelrod, Justin M. Balko, Kelly H. Schlendorf, Robert D. Hoffman, Yaomin Xu, JoAnn Lindenfeld, and Javid Moslehi. “RNA-Sequencing Reveals a Distinct Transcriptomic Signature for Giant Cell Myocarditis and Identifies Novel Druggable Targets.” Circulation Research 129, no. 3 (2021): 451–53. https://doi.org/10.1161/CIRCRESAHA.121.319317.
- Bang, Vigyan, Sarju Ganatra, Sachin P. Shah, Sourbha S. Dani, Tomas G. Neilan, Paaladinesh Thavendiranathan, Frederic S. Resnic, et al. “Management of Patients With Giant Cell Myocarditis.” Journal of the American College of Cardiology 77, no. 8 (2021): 1122–34. https://doi.org/10.1016/j.jacc.2020.11.074.
- Birnie, David H., Vidhya Nair, and John P. Veinot. “Cardiac Sarcoidosis and Giant Cell Myocarditis: Actually, 2 Ends of the Same Disease?” Journal of the American Heart Association 10, no. 6 (2021): e020542. https://doi.org/10.1161/JAHA.121.020542.
- Bobbio, Emanuele, Marie Björkenstam, Bright I. Nwaru, Francesco Giallauria, Eva Hessman, Niklas Bergh, Christian L. Polte, Jukka Lehtonen, Kristjan Karason, and Entela Bollano. “Short- and Long-Term Outcomes after Heart Transplantation in Cardiac Sarcoidosis and Giant-Cell Myocarditis: A Systematic Review and Meta-Analysis.” Clinical Research in Cardiology 111, no. 2 (February 1, 2022): 125–40. https://doi.org/10.1007/s00392-021-01920-0.
- Brailovsky, Yevgeniy, Amirali Masoumi, Rachel Bijou, Estefania Oliveros, Gabriel Sayer, Koji Takeda, and Nir Uriel. “Fulminant Giant Cell Myocarditis Requiring Bridge With Mechanical Circulatory Support to Heart Transplantation.” JACC: Case Reports 4, no. 5 (2022): 265–70. https://doi.org/10.1016/j.jaccas.2021.11.013.
- Cooper, Leslie T., Gerald J. Berry, and Ralph Shabetai. “Idiopathic Giant-Cell Myocarditis — Natural History and Treatment.” New England Journal of Medicine 336, no. 26 (1997): 1860–66. https://doi.org/10.1056/nejm199706263362603.
- Ekström K, Lehtonen J, Kandolin R, Räisänen-Sokolowski A, Salmenkivi K, Kupari M. Incidence, Risk Factors, and Outcome of Life-Threatening Ventricular Arrhythmias in Giant Cell Myocarditis. Circulation: Arrhythmia and Electrophysiology. 2016;9(12):e004559. doi:10.1161/CIRCEP.116.004559
- Fallon, J. M., A. M. Parker, S. P. Dunn, and J. L. W. Kennedy. “A Giant Mystery in Giant Cell Myocarditis: Navigating Diagnosis, Immunosuppression, and Mechanical Circulatory Support.” ESC Heart Fail 7, no. 1 (February 2020): 315–19. https://doi.org/10.1002/ehf2.12564.
- Ghaly, Medhat, Danise Schiliro, and Jadwiga Stepczynski. “Giant Cell Myocarditis: A Time Sensitive Distant Diagnosis.” Cureus 12, no. 1 (2020): e6712–e6712. https://doi.org/10.7759/cureus.6712.
- Gilotra NA, Minkove N, Bennett MK, et al. Lack of Relationship Between Serum Cardiac Troponin I Level and Giant Cell Myocarditis Diagnosis and Outcomes. Journal of Cardiac Failure. 2016;22(7):583-585. doi:10.1016/j.cardfail.2015.12.022
- Heymans S, Eriksson U, Lehtonen J, Cooper LT. The Quest for New Approaches in Myocarditis and Inflammatory Cardiomyopathy. Journal of the American College of Cardiology. 2016;68(21):2348-2364. doi:10.1016/j.jacc.2016.09.937
- Kandolin, Riina, Jukka Lehtonen, Kaisa Salmenkivi, Anne Räisänen-Sokolowski, Jyri Lommi, and Markku Kupari. “Diagnosis, Treatment, and Outcome of Giant-Cell Myocarditis in the Era of Combined Immunosuppression.” Circulation: Heart Failure 6, no. 1 (2013): 15–22. https://doi.org/10.1161/CIRCHEARTFAILURE.112.969261.
- Kociol, Robb D., Leslie T. Cooper, James C. Fang, Javid J. Moslehi, Peter S. Pang, Marwa A. Sabe, Ravi V. Shah, Daniel B. Sims, Gaetano Thiene, and Orly Vardeny. “Recognition and Initial Management of Fulminant Myocarditis.” Circulation 141, no. 6 (2020): e69–92. https://doi.org/10.1161/CIR.0000000000000745.
- Kondo, Toru, Takahiro Okumura, Naoki Shibata, Takahiro Imaizumi, Kaoru Dohi, Hideo Izawa, Nobuyuki Ohte, Tetsuya Amano, and Toyoaki Murohara. “Differences in Prognosis and Cardiac Function According to Required Percutaneous Mechanical Circulatory Support and Histological Findings in Patients With Fulminant Myocarditis: Insights From the CHANGE PUMP 2 Study.” Journal of the American Heart Association 11, no. 4 (2022): e023719. https://doi.org/10.1161/JAHA.121.023719.
- Nordenswan, Hanna‐Kaisa, Jukka Lehtonen, Kaj Ekström, Anne Räisänen‐Sokolowski, Mikko I. Mäyränpää, Tapani Vihinen, Heikki Miettinen, et al. “Manifestations and Outcome of Cardiac Sarcoidosis and Idiopathic Giant Cell Myocarditis by 25‐Year Nationwide Cohorts.” Journal of the American Heart Association 10, no. 6 (2021): e019415. https://doi.org/10.1161/JAHA.120.019415.
- Paitazoglou, Christina, Martin W. Bergmann, Katharina Tiemann, Andrea Wiese, Ulrich Schäfer, Arne Schwarz, Ingo Eitel, and Moritz Montenbruck. “Atrial Giant Cell Myocarditis as a Cause of Heart Failure.” JACC: Case Reports 4, no. 1 (2022): 66–71. https://doi.org/10.1016/j.jaccas.2021.11.007.
- PALMER, HARLEY P., and ISAAC E. MICHAEL. “Giant-Cell Myocarditis With Multiple Organ Involvement.” Archives of Internal Medicine 116, no. 3 (1965): 444–47. https://doi.org/10.1001/archinte.1965.03870030124022.
- Polte, Christian L., Entela Bollano, Anders Oldfors, Anna Dudás, Kerstin M. Lagerstrand, Jakob Himmelman, Emanuele Bobbio, Kristjan Karason, Martijn van Essen, and Niklas Bergh. “Somatostatin Receptor Positron Emission Tomography/Computed Tomography in Giant Cell Myocarditis: A Promising Approach to Molecular Myocardial Inflammation Imaging.” Circulation: Cardiovascular Imaging 15, no. 1 (2022): e013551. https://doi.org/10.1161/CIRCIMAGING.121.013551.
- Sujino, Yasumori, Fumiko Kimura, Jun Tanno, Shintaro Nakano, Eriko Yamaguchi, Michio Shimizu, Nanami Okano, et al. “Cardiac Magnetic Resonance Imaging in Giant Cell Myocarditis.” Circulation 129, no. 17 (2014): e467–69. https://doi.org/10.1161/CIRCULATIONAHA.113.005059.
- Xu, J., and E. G. Brooks. “Giant Cell Myocarditis: A Brief Review.” Arch Pathol Lab Med 140, no. 12 (December 2016): 1429–34. https://doi.org/10.5858/arpa.2016-0068-RS.
- Yang, S., X. Chen, J. Li, Y. Sun, J. Song, H. Wang, and S. Zhao. “Late Gadolinium Enhancement Characteristics in Giant Cell Myocarditis.” ESC Heart Fail 8, no. 3 (June 2021): 2320–27. https://doi.org/10.1002/ehf2.13276.

 Visit Podcast Website
Visit Podcast Website RSS Podcast Feed
RSS Podcast Feed Subscribe
Subscribe
 Add to MyCast
Add to MyCast